

Sudden Cardiac Death in College Athletes
A recent paper on the incidence and causes of death in NCAA athletes over the past two decades made me Stop and Think about making causal connections from anecdotes.

I had thoughts. Maybe you did too.
There were just so many media reports of cardiac arrest in athletes.
This is a column about two things—a medical problem (cardiac arrest) and the way our brains work.
During the pandemic we learned that the vaccine against SARS-CoV-2 could cause myocarditis—or inflammation of the heart. Young males had the highest risk of this adverse effect.
This was neither a welcome finding nor was it a common adverse effect. But it was real. Everyone now agrees. Also well known—from old data—was that myocarditis is a cause of cardiac arrest during sport.
So. When media reports during the pandemic told the dramatic stories of athletes having cardiac arrest, my brain started making causal connections…between a) the fact that most athletes had to take a mRNA vaccine, b) the vaccine could cause myocarditis, a cause of cardiac arrest, c) young athletes, mostly male, had the highest risk of vaccine-related-myocarditis, and d) there sure seemed to be a lot of these media reports.
The cardiac arrest of the famous Danish football star Christian Eriksen added a mental glue to these connections. His cardiac arrest occurred months after the vaccine was released in 2021. There was initial speculation that he had received a vaccine. The director of the team then said that Eriksen was not vaccinated. He is now back playing professional football—with an ICD.
Maybe it was my curated news feeds, but I saw media report after media report of athletes having cardiac arrest. I started to think. Well. That seems like some-thing is going on.
The problem with media reports is that anecdotes do not sum up to data. And now we have some systematic data.
A carefully done paper presented at the recent AHA meeting and published in Circulation found no increase in sudden cardiac death in NCAA athletes. In fact, the authors reported a decline in sudden cardiac death during the years 2021-2022.

This was a 20-year survey in which the authors used 4 independent databases to document the incidence and causes of sudden cardiac death in NCAA athletes.
They found 143 cases of sudden cardiac death over the 20 years. The overall incidence of SCD was 1:63,682 athlete-years, which is inline with published incidence rates from other studies.
Here are the plots of incidence rates over time. You can see a clear decline in the rates over the years. The last two years are the lowest. (Red line.)

The authors also looked into causes of these deaths—a more difficult task. A cause of death could not be determined in 17% of cases.
The most common postmortem finding was “autopsy-negative” sudden unexplained death. This means the heart looked normal on exam. This picture shows the other common causes of death from the autopsy.
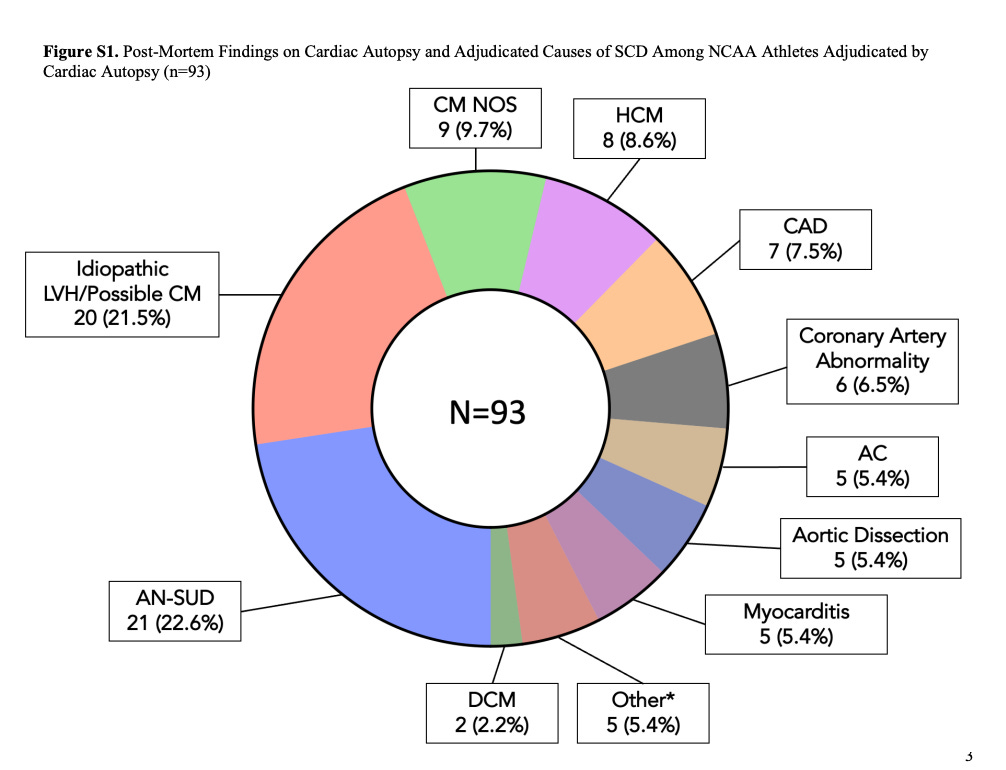

Notably, the authors reported only one case of myocarditis-related death during the 2020-2022 period.
The authors acknowledge limitations. The main one I think is the absence of data on resuscitated arrests. This is important because of the positive trend of increased availability of automatic external defibrillators or AEDs. Namely, it’s possible that there was an increase in cardiac arrests, but not cardiac death—due to better interventions. (In fact, the lower incidence of sudden death in recent years is likely to be due to AEDs).
The Lessons
What I took from this study is to remain vigilant about making causal connections without proper data. Gosh, it seemed like a lot of media reports.
I wasn’t the only one having these thoughts. I recently did a podcast with electrophysiologist Paul Dorian on Sensible Medicine in which we discussed the causes of cardiac arrest in athletes. The post received more than a 100 comments; many writers criticized us for not mentioning vaccine-related arrests.
Yet the lack of any signal of increased sudden cardiac death among NCAA athletes is reassuring. It argues against the idea that mRNA vaccines was causing excess cardiac deaths in young athletes.
This doesn’t mean mandating the SARS-CoV-2 mRNA vaccine in some of the lowest risk groups was a wise decision. In my opinion, the downplay of the myocarditis signal from the vaccine as well as the mandates shredded public trust. It’s a mistake I hope medical leaders learn from.
Yet this study again confirms that anecdotes don’t always sum to evidence. And it is wise to make note of how easy it is for our brains to find causal connections.
Since this is a controversial topic I will allow comments from paid subscribers. If you want to become a paid subscriber, that is great, though I have not put any content behind a paywall. JMM
I appreciate you working at this. However, before you start barking up the wrong tree, you need to look AT the vaccines and their effect, before you can come to the conclusion that the vaccines weren't part of the picture. Your conclusion is rather premature; this is again a poor use of epidemiological research to prove a point before you can reliably make it in any empirical sense. Again again we see this -- it's a bad faith use of statistics. You're extrapolating several levels that you definitely cannot say for sure. Why does everyone insist on doing this? You should be asking more questions, not pretending like you have answers.
The paper itself, when not abused to make your point, has some extremely interesting findings. For instance: Eight cases of death were attributable to myocarditis over the study period (1 case from January 1, 2020, through June 30, 2022), with none attributed to COVID-19 infection.
That's really interesting, way more interesting than any of the points you make. I'll just leave it there for contemplation.
I wrote a paper when I was a fellow about the sudden death in the Air Force over 20 year review that was published in JAMA . We did have four deaths due to myocarditis specifically smallpox . We even had electron micro graphs. I still have a few showing smallpox virus in the heart of the athletes. Over the years, the military has reported outbreaks when they use the particularly nasty batch for the vaccine. They were vaccinating the soldiers day 1 and they would be at risk at day seven when they were doing PT. It is no longer an issue because they do not use live virus. I actually went to the Armed Forces epidemiology board in Washington DC to talk about the risk benefit analysis of continuing to use smallpox vaccinations, knowing this would happen. it was felt that the threat of bioterrorism debilitating our armed forces was greater than the risk of death, which was real from smallpox myocarditis . Overall, there were 17 patients with structural heart disease, including some pretty complex disease that was missed during the screening process. Several people had no overt cause . It worked out to one death for every 5 million hours of exercise. Interestingly, you were far safer to be an Air Force recruit in basic training than to be a young adult driving cars etc. outside of the military. It is extraordinarily safe environment. The history of getting it published was fascinating. I was working at the Armed Forces Institute of pathology during my fellowship when a young adult came in who died suddenly. Dr. Virmani, a well-known cardiac pathologist asked with Dr. Rabinowitz, her partner that it would be nice if we knew the actual incidence of sudden death. I said I knew it was one and 60,000 athletes . They said, how did I know- I said it's how many basic trainees go through a year and we had one death per year they wanted to know if that data was anywhere published. Turns out a secretary had a file of every single death, cardiac and non cardiac with complete autopsies on every airman over 20 years. The military had not wanted it published because even though it was an extremely safe environment, they felt it was bad press. Eventually a Gen who was an internist said to me go ahead it seems like this is good data and the approved publication. What was fascinating was the public health strides over the years and if I had more energy I would write about it. They were seeing lots of young troops, die of infectious disease being put in the barracks. We were actually taught how to do transtracheal aspirations in these young adults to get clean sputum samples to culture out these weird bugs. Eventually, it was a medical resident who suggested giving everyone measles, mumps, etc. vaccines because some of these kids came from areas of the country they were never ever vaccinated Once the vaccination program started a lot of these illnesses resolved. They were seeing heat related deaths. We had a code red and would put people in ice baths. That prompted the red flag criteria which based on the heat temperature index prevented exercise on hot days or started the exercise as we used to say at O dark 30 at three in the morning . It was a very interesting time, but the military medical system eventually made it a very safe environment for these young adults to come and go into training.