
Chapter 2 of my Paul Wood Lecture
Chapter 2 of my Paul Wood Lecture
In the second act of my talk I describe the historical lesson from preventive hormone replacement therapy in post-menopausal women.

During my medicine clinic as a resident at Indiana University in the 1990s, I prescribed hormone replacement therapy to post-menopausal women. The goal was not to alleviate post-menopausal symptoms; instead, the goal was prevention of future cardiac events. (I have now developed an allergy to preventive—anything.).
Two reasons drove the enthusiasm behind preventive HRT. First was plausibility. Pre-menopausal women have super-low rates of cardiac events. Female hormones must be the protective cause. So we can just give them to older women and achieve the same benefits enjoyed by younger women.
The second reason behind HRT were studies like this one. In 1992, the prominent journal, the Annals of Internal Medicine, published a systematic review of more than 30 studies of HRT in older women.
Here is a series of slides:
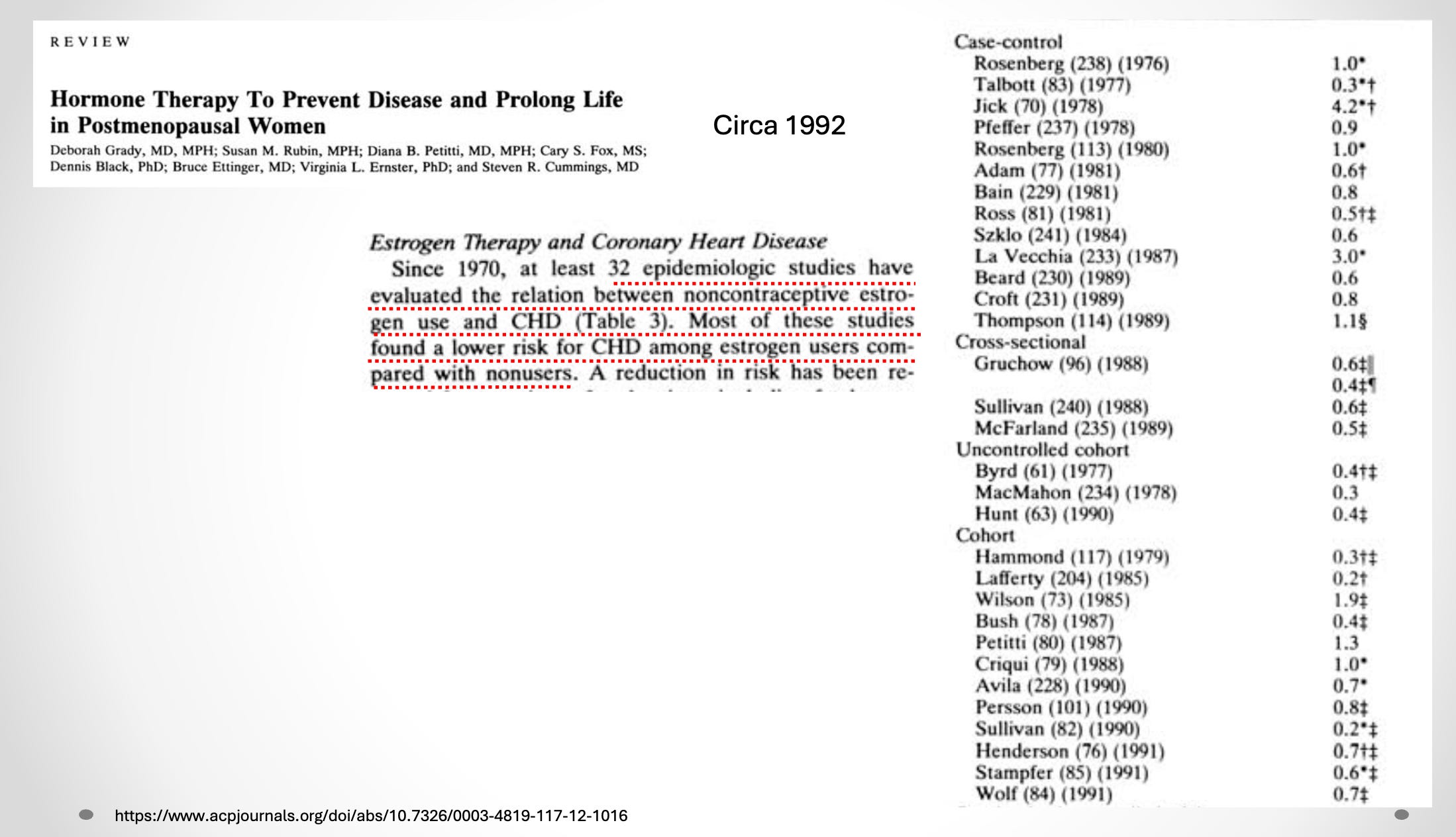
In the right column are the studies. When the decimal is below 1.00, the study found that women who took HRT had lower rates of coronary heart disease. None of these studies were randomized trials.
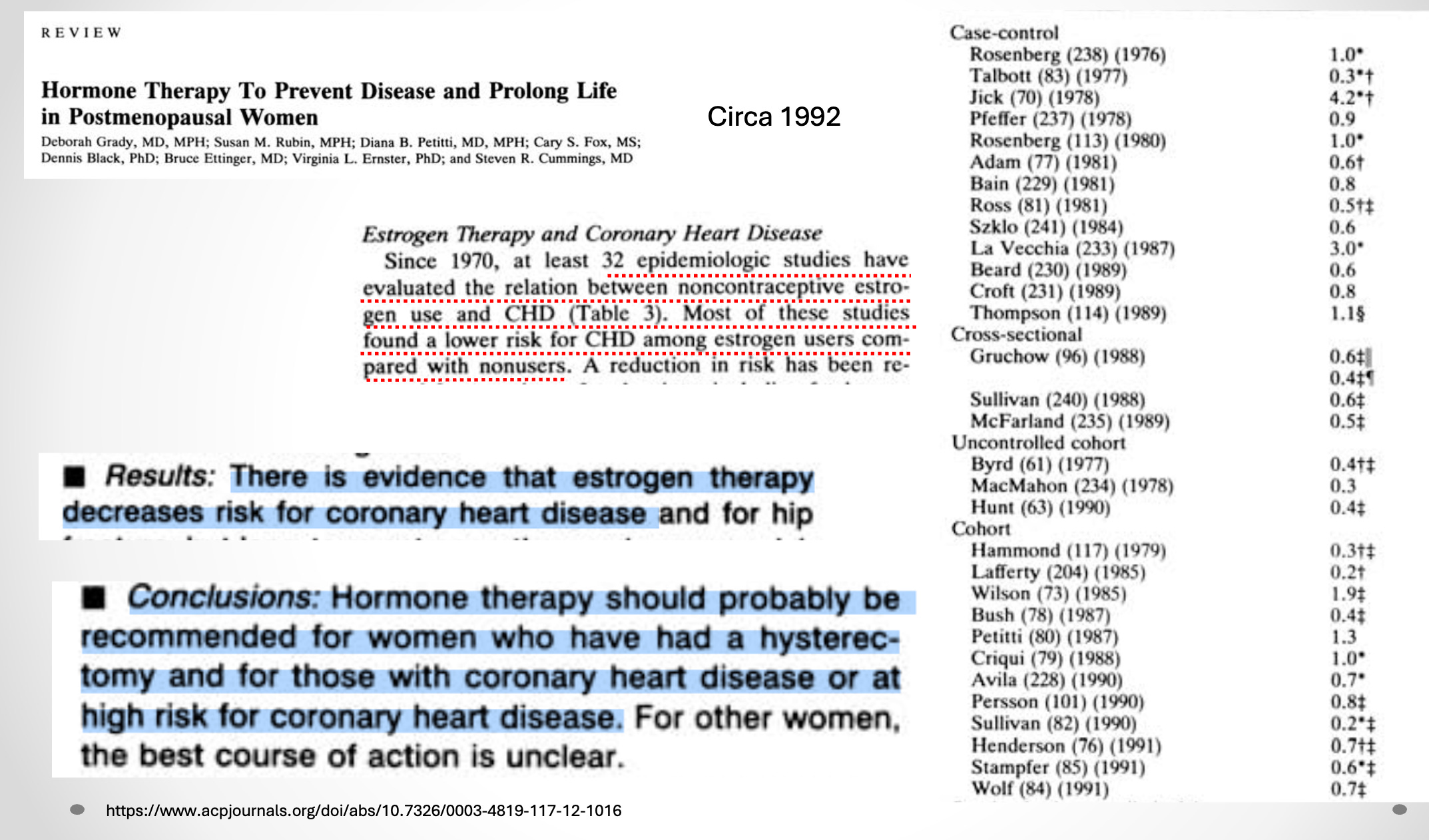
There were so many of these studies that the authors used causal language to describe the relationship between hormones and lower rates of events. See highlighted text in the next study. Note the causal verbs.
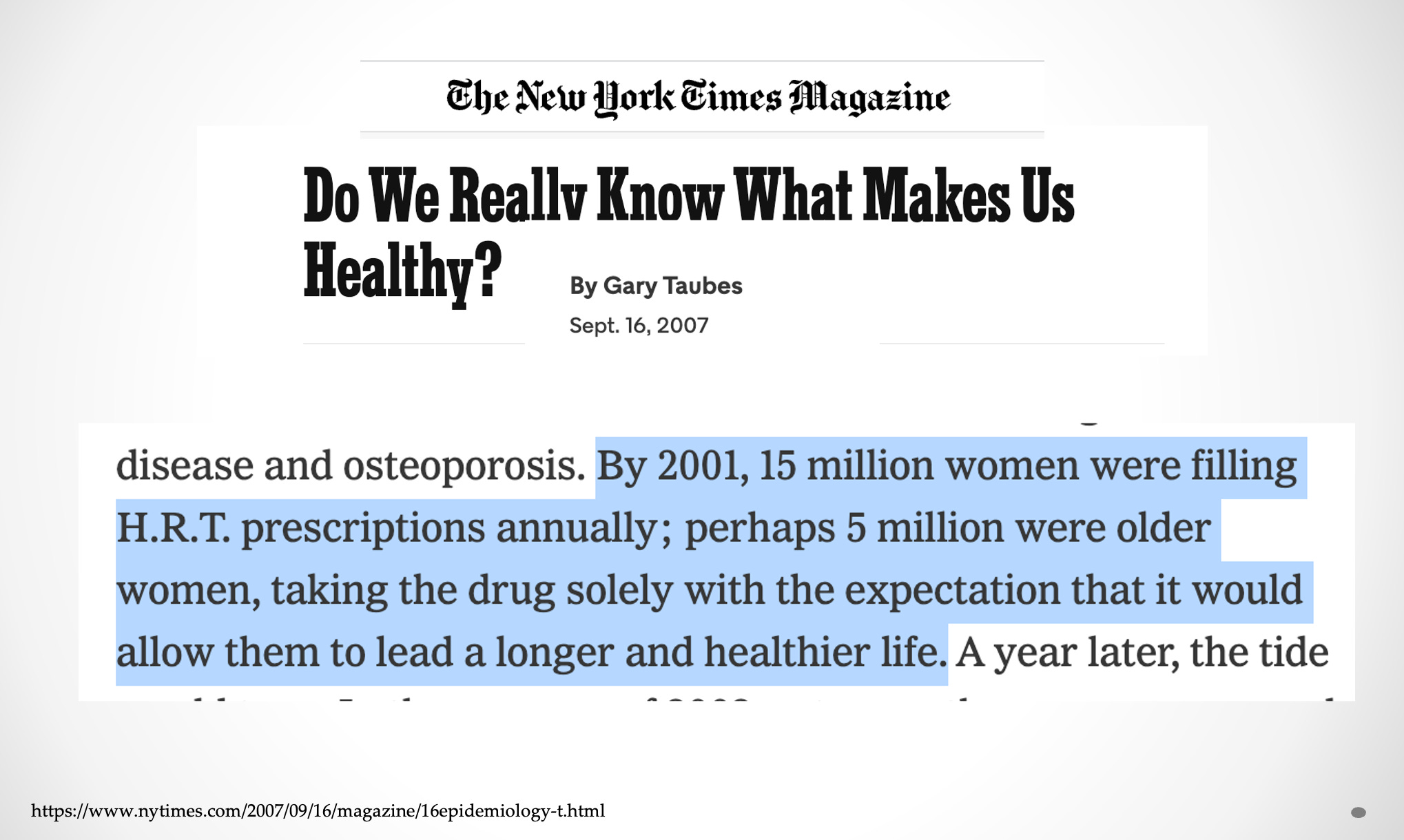
Ten years later, Gary Taubes wrote in the New York Times that millions of women took these drugs for prevention. Causal language had persuaded doctors and patients alike.
Then came the shocker. JAMA published results of the Women’s Health Initiative trial. More than 16,000 menopausal women were randomized to HRT or placebo.
The results showed that expert consensus was harming women.
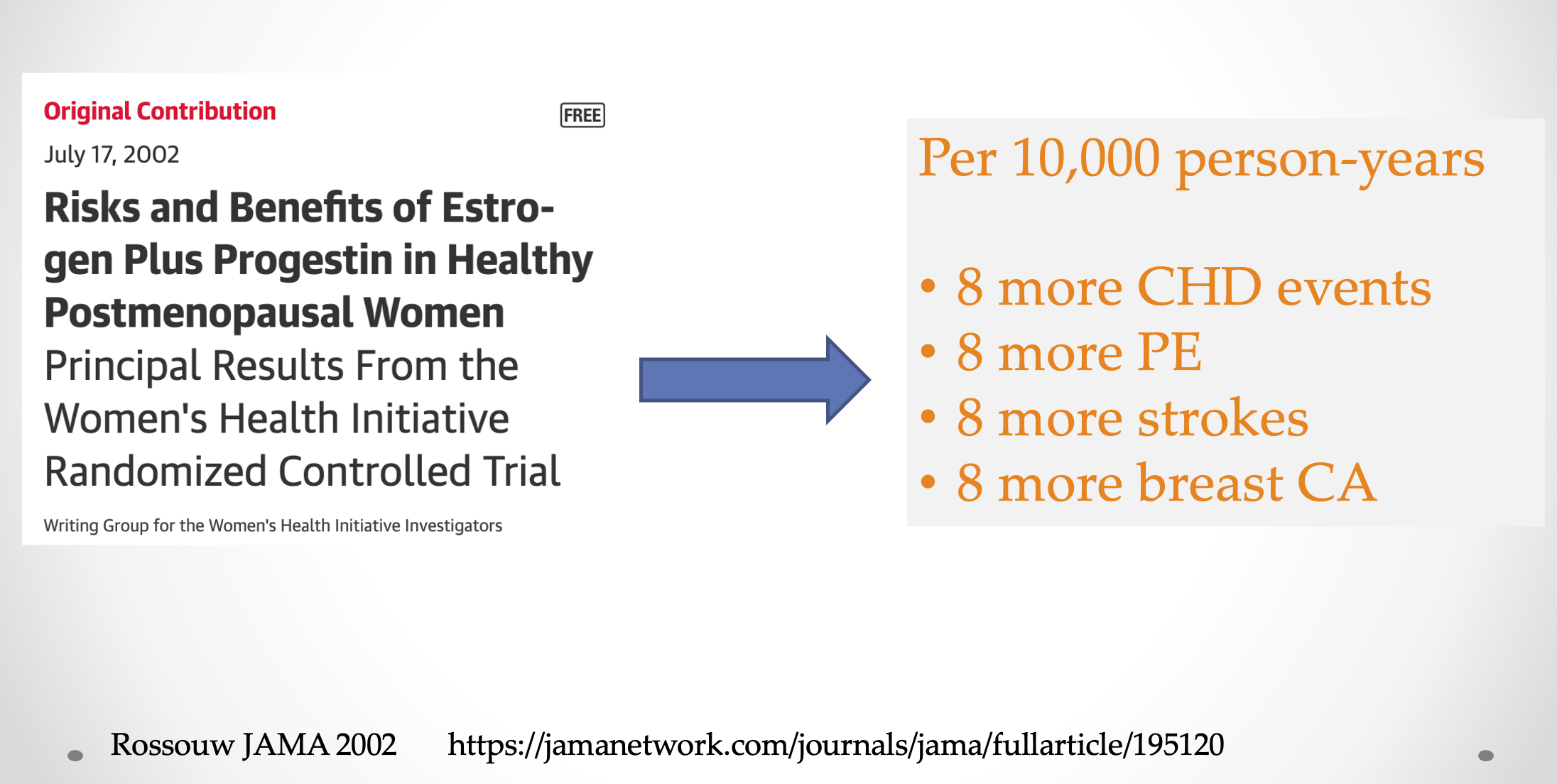
Let me repeat: expert consensus caused harm.
There were caveats and important things to consider in translating this evidence. This report emphasizes how an RCT reversed years of observational data and expert opinion. What I was taught to do in the IU medicine clinic was dead wrong.
The famous Peter Attia, MD has criticized WHI. He rightly notes that WHI enrolled older women (age 62), used older forms of HRT and revealed small absolute risks from HRT. All of these things are true. Timing, duration and type of HRT are all relevant considerations.
My point in exploring this massive reversal is not to convince you that HRT is always bad.
The point of this story is that something we did for prevention, for decades, caused harm. And. At the heart of this mistake was overconfidence in observational data.
Observational data can be useful. You can even determine cause and effect from observational data. Smoking was shown to cause cancer without an RCT.
In the case of HRT, we did not realize that non-random comparisons between women on HRT vs those not on HRT were marred by bias. When there is a systemic bias, it does not matter if there are 30 or 300 studies. Or 300 patients or 3 million patients.
The preventive HRT reversal underscores the importance of the randomized trial. This story makes me stop and think. That is why I used it in the Paul Wood lecture in Manchester. JMM
A fundamental lesson in methodology, a cautionary tale about primum non nocere, and the ready-made push back against the hubris of biological plausibility, all rolled into one. And WHI is the gift that keeps on giving. Recent evidence from the estrogen-only RCT portion shows a real (albeit small) increase in ovarian cancer risk.
And yes, WHI doesn’t answer everything. Perhaps the women started HRT too late. Perhaps they took HRT for too long. Perhaps modern estrogens rather than CEE might have different results. All perfectly fine speculation. And if there’s one thing to take away from WHI, it’s STFU with the speculation, and for any proponents to go out and prove it.
Seatbelts, sober driving , not smoking anything , being at ideal body weight, walking or exercising a bit and laughing probably the best you can do . That and an ldl under 70